
Talking about lungs, lung nodules are described as “spots” that are 3 centimeters (1.5 inches) in diameter or less (lesions larger than 3 cm are referred to a lung masses. Lung nodules are very common, especially in people who have smoked, but not all lung nodules mean lung cancer; there are many possible causes.
Human detection of growths is done by an important biological procedure called biopsy which is a basic procedure that is subsequently led after the restorative examinations by master radiologists. The biopsy is an examination of tissues removed from a living body, to discover the presence of a disease and the process is nearly invasive.

On a different note, Interstitial Lung Disease (ILD) is a general category that includes many different lung conditions. All interstitial lung diseases affect the interstitium, a part of the lungs’ anatomic structure. The interstitium is a lace-like network of tissue that extends throughout both lungs. By medical imaging empowered by the new research in Computer Vision, patterns are segmented in the HRCT images of the interstitium to diagnose cases of ILDs.
In the context of the AI systems built by Prof. Mukhopadhyay and team, the first system will work as an AI assistant to help the radiologists distinguish between malignant and benign lung nodules. The other system will help recognize interstitial illness patterns in HRCT pictures delineating the lung tissue surface. Computer imaging makes these procedures non invasive.
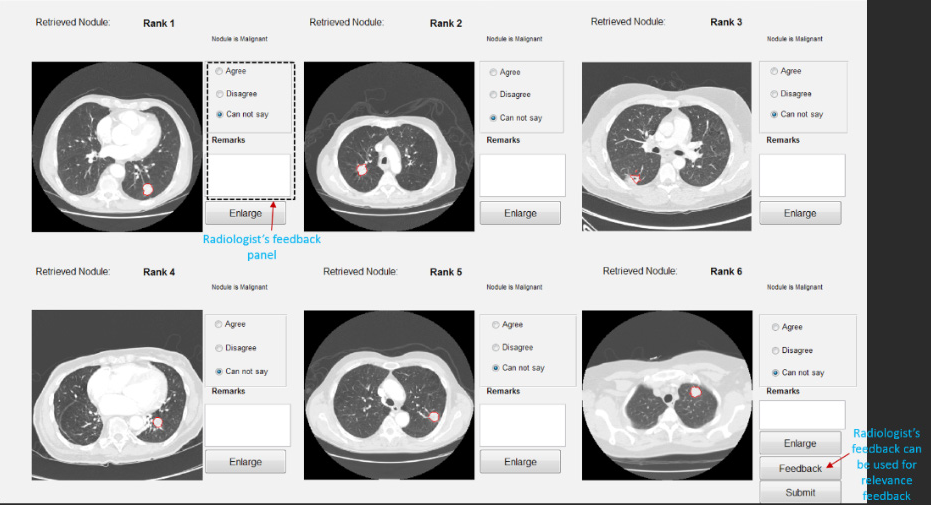
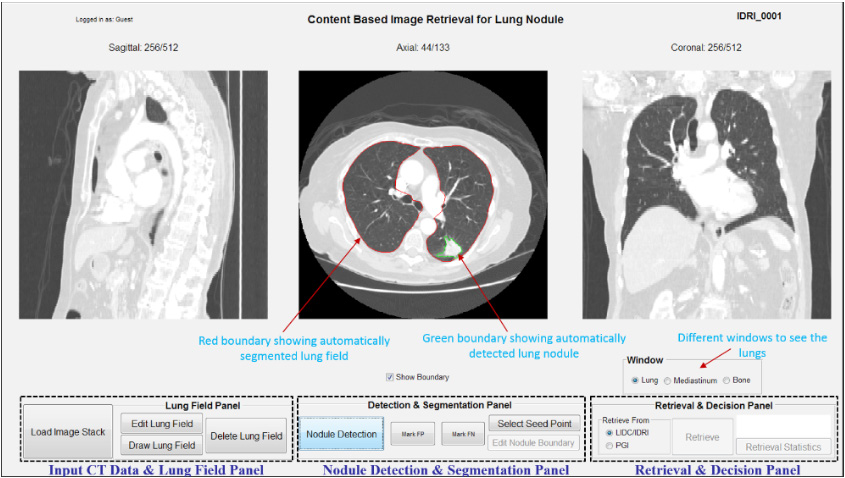
For the first AI system- Lung CAD that categorises lung nodules as benign or malignant, the workflow is as this- First, it identifies the Lung nodule, then segments the nodule, and then paves the way for improving the segmentation. Next, the procurement of information for skin nodules takes place from the database and their report is judged for the probable malignancy. The query nodule in further cases is analyzed on the basis of these retrieved results. However it must be kept in mind that Lung CAD is a secondary assistant to the Human radiologist and serves primarily as a confirmatory source.
Interestingly, Lung CAD has another important application- the training of new radiologists. The AI System can be trained on the judgement of the expert radiologists and new radiologists can compare their conclusions with that of the system to understand the ideology of the established radiologists.
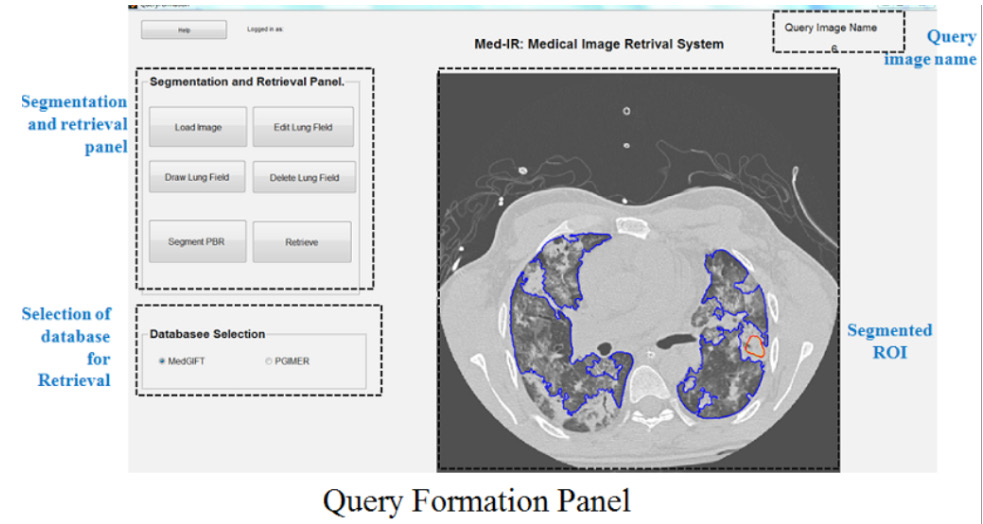
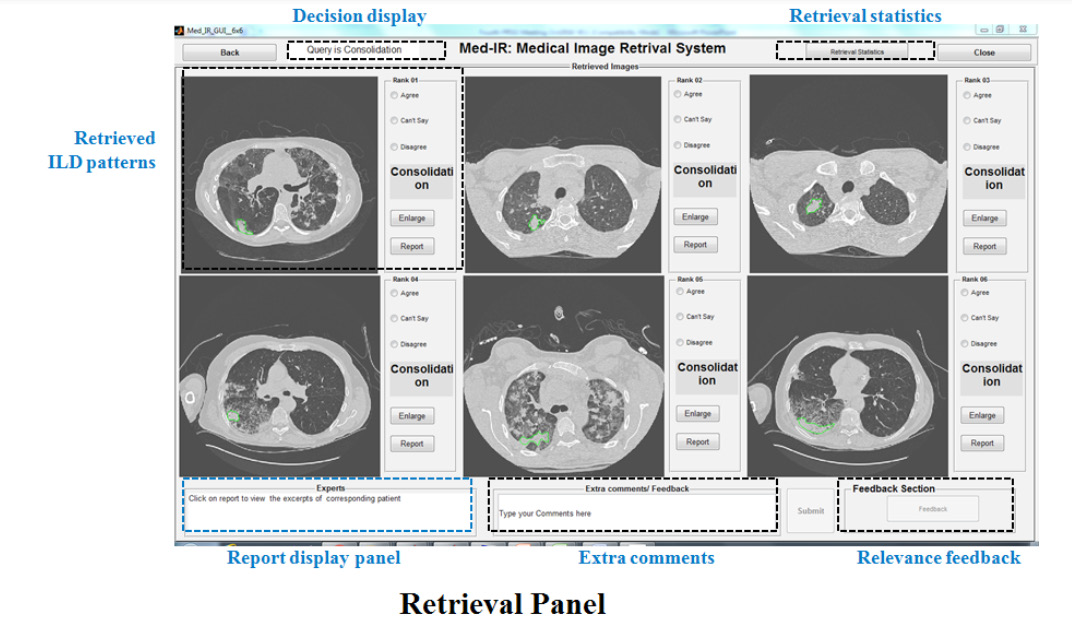
Coming to the second AI system- the ILD detector the workflow goes as- automatic segmentation of the pathological region within the lung area followed by imparting flexibility to decide the boundary of the same and then acquiring similar behavioral segments from the database to finally assess the probability of the pathological segment to fall in a particular ILD category as concluded from the processed results. The final verdict regarding the suspected disease is proclaimed by doctors on the basis of the spotted ILD pattern and the gathered clinical information.
The suitable test site required for the validation of both the AI systems was provided by AIIMS Delhi, wherein the softwares passed the test with flying colors. Lately, lung nodule detection rate and grouping rate has been 86% and 87%, respectively, and the achievement rate for ILD classification: 84%, as provided by the researchers. The team of researchers has been progressing in the direction of further upgrades so as to lead clinical preliminaries on wider samples.
Even radiologists from PGIMER Chandigarh extensively supported the research throughout by providing the required clinical information, inclusive of the biopsy cases reports and testing the software for a prolonged duration. For the full-proof testing of the decision system, it will go on for a clinical trial in 3 places across India and if qualified, the prospects for market capitalization will be able to embrace the research.
Interestingly, the AI systems are sensitive to the country of the Training Image dataset , for example, the restorative image scan database utilized for reference belongs the Indian patient population. In the process of developing the System, it was conclusive that the public database from the US: LIDC-IDRI and MedGIFT ILD (built utilizing the data from University Hospitals of Geneva) gave poor results when tested on Indian population and vice versa! The number of false positive cases observed were significantly high to be ignored.

“The mismatch perceived due to change in the datasets could be because of the racial variations or disparity in terms of interpretation of the cases by the radiologists of different countries”, said Prof. Mukhopadhyay.
The commercial aspects of the two systems however looks quite different. Lung CADs have been in the mainstream medical technology for a long time since 2002. This sector already has established players like Philips and Siemens who have oligopolized completely. As a matter of fact when Prof. Sudipta Mukhopadhyay started with the research in this particular field, it was expected that the literature available for their research would be plenty as Lung CADs have existed in the market since 2002.
Contrary to this expectation he could barely find any profound research papers! “The tech giant companies: Philips, Siemens and Insight manufacture these devices worldwide and have been prospering in this business arena for quite some time. The chances that they even capitalize on the research catering to lung CADs through their collaboration with Universities is probable. It’s quite evident that these tie-ups and the imminent Non Disclosure Agreements become the reasons behind scarcity of enough accessible research papers catering to the field of lung CADs.” added Prof. Mukhopadhyay.
On the other hand commercialization of the ILD Detector System is very feasible, there hasn’t been much established research and equipment development in this area. The novelty of this software lies in the lack of commercialized products pertaining to this research hence portraying the exclusivity of this technology to detect Interstitial Lung Diseases.
Prof. Mukhopadhyay added as a side note “With the upcoming instances of malignant growth of pulmonary nodules and other respiratory illnesses in India, the requirement for skilled radiologists just tends to increase with time.” The lung CAD built will merely serve as the personal assistant to the radiologists, enabling them to proofread their interpretations with the help of developed software.
The stress on the requirement for skilled radiologists can not be made enough for revolutionising the ambit of Lung Disease diagnosis.
Written By Shreya Santra
Special thanks to -Dr. Ashish Kumar Dhara, Shrikant Mehre (Lung CAD, CT Images) - Dr. Jatindra Kumar Dash, Mandar Kale (ILD Patterns, HRCT Images)
